

| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Original Article
Volume 4, Number 1, March 2015, pages 173-177
Arginine as a Significant Regulator of Supersaturation in Calcium Oxalate Lithiasis: the Physiological Evidence
Stoyanka Slavcheva Atanassova
Department of Clinical Laboratory and Clinical Immunology, Medical University, Sofia 1431, Bulgaria
Manuscript accepted for publication February 17, 2015
Short title: Arginine as a Regulator
doi: http://dx.doi.org/10.14740/wjnu199w
| Abstract | ▴Top |
Background: At present, the possible effect of arginine as a natural regulator of calcium oxalate (CaOX) supersaturation and crystallization in human urine has been analyzed.
Methods: Two types of experiments have been discussed: clinical laboratory analysis on the urine excretion of arginine (Arg) in patients with CaOX lithiasis and detailed measurements of the kinetics of the dissolution of CaOX calculi in artificial urine, containing various concentrations of Arg.
Results: A detailed analysis showed that 80% of stone formers (SFs) eliminated pathological values: 30% of patients had lower plasma levels compared to controls and about 50% of SFs showed higher concentration. Urine concentrations in these two groups were not reported.
Conclusions: The in vitro analytical measurements demonstrate even a possibility to dissolve CaOX stones in human urine, in which increased concentration of Arg has been established. Discussions have arisen to use increased concentration of Arg in urine both as a solubilizator of CaOX stones in humans and on the purpose of a prolonged metaphylactic treatment.
Keywords: Calcium oxalate calculi; Arginine; Dissolution of crystalline; Urine supersaturation
| Introduction | ▴Top |
The interest towards the formations of renal calculi can be explained by the wide speard of nephrolithiasis [1, 2] and that kind of stones is caused by some gastrointestinal diseses [3, 4]. Despite a number of promising hypotheses, the pathogenetic mechanism of the intrarenal calcium oxalate (CaOX) stone formation remains obscure; thus the clarification of the main physico-chemical moments of the processes of phase formation in human urine is of significant clinical importance.
In investigating the kinetics of crystal nucleation and growth, and the kinetics of the dissolution of already existing stones, of utmost significance are the issues related to the calculation of the level of supersaturation in biological solutions (such as urine). The urine’s saturation is the driving force for the formation of the calculi and still cannot be regulated. In this conection, the results of this study could be put into practice in the clinical treatment of stone formations.
Of all the stone forming substances in the human urine, of most significance is the CaOX precipitation, both, because of the dissemination of the CaOX urolithiasis and because it is the most insoluble stone former (SF). It has to be noted that, in view of the dominant role of hypercalciuria in the pathogenesis of calcium stones [5-7], our therapeutic efforts in respect to those factors are neither clinically, nor scientifically satisfactory.
In recent years, it was shown that the supersaturation in the urine is determined not so much by the concentration of the ions (Ca2+ and C2O42-) constituting the concrements, but by the presence or absence of complex forming agents in the urine. It has been evident since Hammarsten’s classic studies [8] that many ions, such as Mg2+, citrate or HPO42-, which are normally present in the urine, increase the solubility of CaOX in aqueous solutions by forming complexes with either the Ca2+ or the C2O42- ions. However, the oral administration of these complexing agents does not lead to encouraging clinical results, as they metabolize quickly in the organism.
There has been an increasing interest, particularly, in Ca-binding amino acids, due to their role in many calcium-dependent physiological processes. The possible inhibiting impact of various amino acids (alanine, ornithine, tryptophane, etc.) on the type of the CaOX formation and on the subsequent CaOX growth in the urine is often discussed in academic literature. The above mentioned amino acids, which are also common in the urine, have an inhibiting effect on the CaOX growth even at minimal concentration [9-11].
According to our in vitro data [12], arginine (Arg) is a weak complexing agent with respect to calcium. Arg (C6H14N4O2) is present in the human urine at lower concentrations relative to other amino acids; its urine’s excretion is 7.0 - 47.0 μmol/24 h [13]. We found that in physiological solutions, resembling the human urine in their composition, the complexing effect of L-Arg with respect to Ca2+ ions was surprisingly higher. Those preliminary results and the possible biological significance of Arg provided the impetus for a thorough examination of the kinetics of the CaOX concrements dissolution in physiological solutions containing various concentrations of acid.
Up to now, no analysis has been performed on the possible correlation between the Arg’s concentration in the urine and the inclination to develop CaOX calculosis. The results obtained in our in vitro experiments [12] regarding the dissolution of CaOX in physiological solutions, containing an increased concentration of Arg, stress the importance of those analyses.
| Patients and Methods | ▴Top |
Two types of experiments were performed in the framework of this investigation: 1) analysis on the concentration of the Arg in serum and urine in patients with CaOX stones, as well as, in a healthy control group; and 2) an investigation on the kinetics of dissolution of CaOX calculi in physiological solutions, containing various concentrations of Arg.
Patient studies
SFs
Fifty-six patients (30 men and 26 women) were included, whose age ranged from 14 to 65 years, at the beginning of the calculosis, and who had had their CaOX renal calculi removed spontaneously, by surgery or through extracorporeal shockwave lithotripsy (ESWL). Each patient had a known clinical and family history of this disease, including data for episodes of a renal colic and of concrements elimination, the presence of metabolic disorders and so forth. During the conduction of the study, the patients were on free diet and fully compensated renal function. They did not report any liver disease.
Controls
Fifteen healthy subjects were included who never had any urological and hepatic trouble.
Calculi
The calculi were taken at random from patients who had undergone surgical or ESWL removal of the stones.
Methods
A 24-h urine collection was obtained from each patient. During the period of urine collection, specimens were refrigerated and aliquots of the 24-h volume and sample were immediately frozen until analyzed. The volume of urine in every sample was recorder on completion of the collection and pH was measured by using a glass electrode pH-meter.
Serum was obtained from the same patients as those whose urine was collected from. Heparinized plasma was separated by centrifugation and was also stored at temperature -25 °C.
The amino acid (Arg) contents of the sample were determined using a Hewlett Packard HPLC 1050, coupled to a fluorescence detector. Ethyl alcohol was added to the urine specimens to allow the precipitation of proteins and the extraction of free amino acids. An automated precolumn orthophtalaldehyde derivation procedure was employed. Separations were done using a reversed-phase column (Waters Corp). Amino acid concentration of the samples was determined by comparison with values obtained from a standard curve. Amino acid concentrations are expressed in µM.
The amino acid (Arg) in urinary calculi was evaluated as follows. The calculi were carefully rinsed in saline to remove any contaminations (blood clots, etc). The calculi were dried with filter paper and ground into a powder in an agate mortar. To 0.5 g of the powder, 4.5 mL 90% ethyl alcohol were added, well mixed and left for 10 min to allow the precipitation of proteins and extraction of free amino acids and then centrifuged. The supernatant was evaporated to dryness under vacuum at a temperature not exceeding 55 °C. The residue was re-dissolved in 0.2 mL 10% isopropyl alcohol. The qualitative analysis of the calculi was carried out by the HPLC.
Statistical analysis
Statistical analysis of the data obtained from both the SF patients and from the control group was performed using Student’s t-test to establish the significance of the difference between mean values. All results were expressed as mean ± SEM and the differences were considered significant if P < 0.05.
Dissolution of CaOX concrement: basic theoretical considerations
Human urine is a complicated physiological solution. The physic-chemical formalism of the kinetics of dissolution of kidney stones has been developed, in details, in our papers [14, 15]. One can see that simple formulae can be obtained, describing the effect of complex forming agents (present in the solution at various concentrations) on supersaturation, solubility, and growth velocity of CaOX crystals growing or dissolving in solution, resembling human urine. It can be shown that if we introduce an increasing concentration CArg (e.g. L-arginine) of a Ca2+- binding complex forming agent, having a solubility constant KArg into the solution, a linear dependence between the solubility SArg and CArg for Ca2+ >> C2O42- can be predicted by:
SArg= S (1 + KArgCArg/α’) (1)
where α’ is the α factor in the absence of the complex forming agent “Arg” (here indicating L-arginine).
Thus, the dependence of the supersaturation Δμ on CArg for the physiologically significant case Ca2+ >> C2O42- , determining the supersaturation in urine is:
Δμ ≅ Δμo - 1/2ln (KArgCArg/α’) (2)
where Δμo is the supersaturation in respect to the CaOX-precipitation without Arg added.
It is also of interest that in the case of the dissolution of CaOX concrements in the presence of a fixed initial concentration of CaOX (or, which in the case of Ca2+ >> C2O42- is the same, in the presence of constant concentration Co* of oxalic anions) we have to rewrite (1) as follows:
SArg = S (1 + KArgCArg/α’) - Co* (3)
Thus a plot of SArg versus CArg should result in a straight line with a slope of -SKArg/α’, cutting from the ordinate axis a segment SArg (O) = S - Co*. In this way, both SArgand KArg can be determined at a known value of α (according to data in Robertson et al [16], α’ in human urine is approximately 2).
Thus, depending on the concentration CArg, that is, on the sign of Δμ (i.e. Δμ > 0 during growth, Δμ < 0 during dissolution), growth or dissolution of CaOX concrements can be achieved simply by changing the concentration CArg of the Arg added.
Instrumental techniques
The experiments on the kinetics of the dissolution of CaOX renal calculi were performed in Jena glass round bottom flasks thermostated at 25 °C. The volume of the studied solution was 1,000 mL and it was stirred (about 200 rpm) by an electromagnetic stirrer. The Archimedean weight G (t) of the samples of CaOX calculi, put in a platinum net basket and suspended to a torsion balance, was continuously measured with a sensitivity of ± 0.5 mg [14, 15].
The CaOX calculi used had been formed in the urinary tract and eliminated spontaneously by the patients. The calculi were selected to have a weight of 100 to 200 mg and to be of identical mineral composition, mainly CaC2O4.2H2O (weddellite). The composition of the calculi was checked by polarized-light microscopy and thermogravimetry (DTG).
We employed two different types of aqueous solutions, mimicking urine [17, 18], with our solvent (Arg) introduced in several different concentrations.
| Results | ▴Top |
Clinical laboratory data
Table 1 [13] shows the plasma levels (µmol/L) and the urine excretion (μmol/24 h) of amino acid Arg in the groups of the patients (SFs) and control subjects. A mathematical estimation of the deviation from the observations on amino acid in patients has been made.
 Click to view | Table 1. Serum Levels and Urine Excretions of Amino Acid Arginine in the Patients With a Calcium Oxalate Calculosis and Control Group [13] |
Thus, plasma levels of Arg in the patients were non-significantly higher compared to those of a control group. A detailed analysis shows that 80% of SFs eliminated pathological values: 30% of patients had lower plasma levels compared to controls and about 50% of SFs showed higher concentration.
Urine concentrations in these two groups were not reported.
Data of in vitro experiments
The solubility of CaOX in artificial urine with zero supersaturation is considerably increased (8.7 × 10-5 mol/L) compared with its solubility in pure water (5.5 × 10-5 mol/L) due to the presence of complexing ions (Mg2+, citrate ions, etc.) in this solution as predicted by αi coefficients known from an analytical chemistry [8, 14]. When L-Arg is introduced into the same physiological solution, a dramatic change in solubility (up to 55 × 10-5 mol/L (i.e. about 70 mg/L) is observed, as shown in Fig. 1.
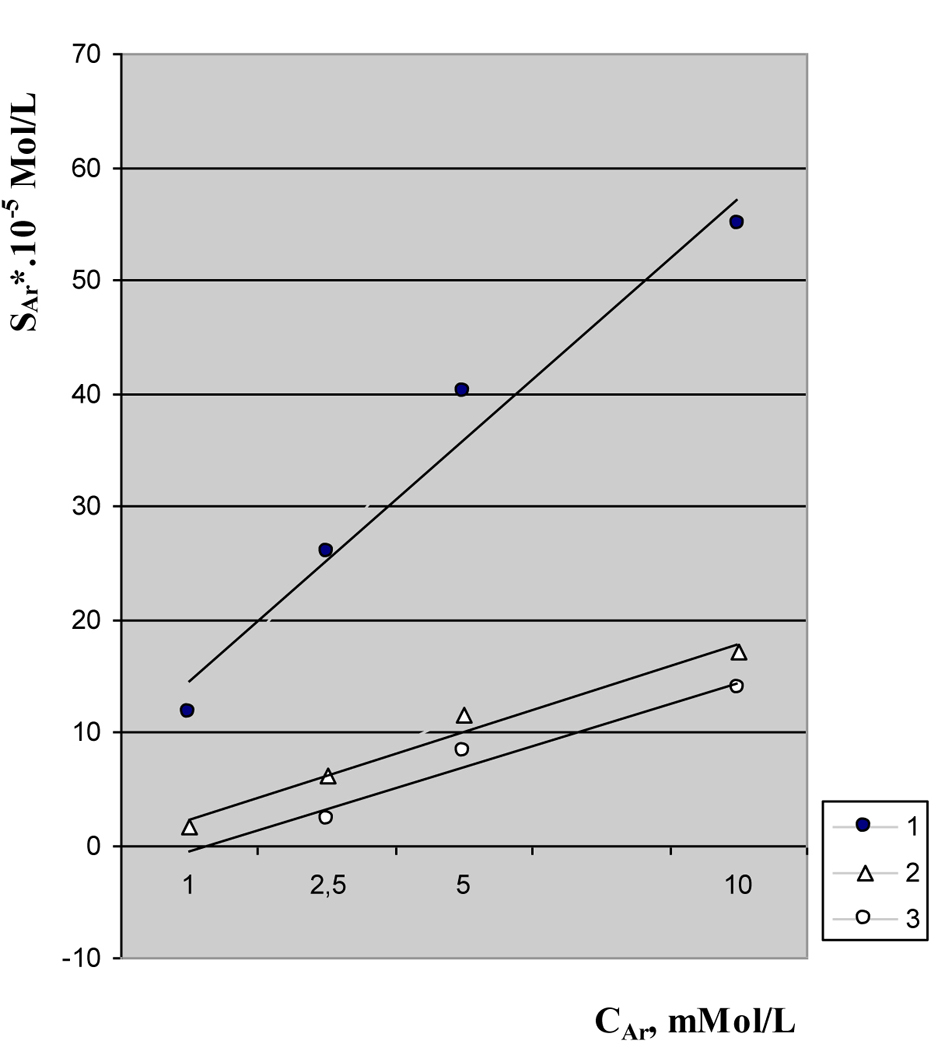 Click for large image | Figure 1. Solubility of calcium oxalate calculi in artificial urine as a function of L-arginine concentration. Solubility in zero saturation urine (curve 1). Solubility in artificial urine with lower saturation (curve 2). Solubility in artificial urine with normal saturation (curve 3). |
A similar effect of L-Arg is also seen in artificial urine, in which distinct supersaturation (due to the presence of a normal concentration of Ca2+ and a medium concentration of C2O42- ions [12]) has been maintained (Fig. 1, curves 2 and 3).
In accordance with Eq (1), a linear dependence of the solubility on CArg is observed (Fig. 1) for each series of measurements, in which three different supersaturation values (zero, medium and normal) have been established. The effect of the increasing concentration of L-Arg on the solubility of CaOX crystals is clearly evident; the initially supersaturated solutions are transformed into undersaturated systems. The effect of the presence of Ca2+ of the course of the straight lines 2 and 3 in Fig. 1 when compared with the no-Ca2+ case (line 1 in the same figure) is to be noted. A sharp decrease in the slope of lines 2 and 3 is observed, too. Since the two solutions have the same Ca2+ concentration, curves 2 and 3 are parallel, as expected from the formalism, as discussed above [14].
| Discussion | ▴Top |
This paper examines the role and place of the amino acid Arg in the pathogenesis of CaOX renal calculosis. It has been found that Arg is a very effective solvent of CaOX calculi in solutions characterized by the composition and ionic strength of human urine. We have found that the mechanism of dissolution of CaOX calculi follows the Nernst model of a diffusion-limited process as it is discussed in detail in literature [12, 14, 15]. The dissolution of CaOX with Arg is a relatively slow process, taking approximately 1 month to dissolve about a 70 mg sample at zero supersaturation. Detailed analysis performed in our study indicates that Arg is comparable, in its solubility effect, to the best known classical complex binders of Ca2+ or C2O42- ions in urine, that is, Mg2+ and citrate anions. This can be seen from Table 2 [8, 14, 16], in which the stability constant KArg of Arg calculated in our results (Fig. 1, Eq. 1) is compared to the Ki values of Mg2+, Na-EDTA, and other known complex-formers of CaOX.
Click to view | Table 2. L-Arginine as a Solvent of Calcium Oxalate: Comparison With Classical Complex Forming Agents [8, 14, 16] |
Arg is one of the amino acids constituent of normal human urine. Arg is found in all proteins, which means that it is necessary for life. From bases and arginaza enzyme, which is found in the liver, it breaks down into urea and ornithine (ornithine cycle). The addition of Arg can reduce the binding of free radicals in tubular membranes, respectively to reduce nephrocalcinosis [19, 20].
Insignificantly higher are the serum levels of Arg ((NH)2C(NH2)CH2CH2CH2CH(NH2)COOH) for the patients to a CaOX lithiasis compared to control group. Of all finded free amino acids in CaOX stones, Arg is amino acid with highest frequency - 21.6 nmol/mL. But do not expect that fact alone may explain the lack of Arg in urine collections. One possible explanation of this is the disintegration of the acid by the action of the enzyme arginaza to ornithine (H2NCH2CH2CH2CH(NH2)COOH), i.e. we cannot consider separately excretion of ornithine from Arg’s metabolism. On the other hand, free acid ornithine is not detected into the proteins, i.e. it is the main “body” of the amino acid Arg. Ornithine is the amino acid with a clearly complex action [21] and in this context, lower urinary excretion of ornithine (more than 60% of patients [22]) may explain low inhibitory activity of urine of these patients. From the analytical chemistry, it is known that the ornithine is an agent forming complex compound with metals (for example, calcium) leading to lower levels of urine saturation in unaffected patients.
Arg was not detected in the urine of patients with CaOX stones. The absence of this acid in groups of CaOX-SFs is of great interest, especially in light of non-difference Arg levels in the plasma of SFs and controls. More so than 30% of patients with CaOX stones have significantly lower plasma levels of Arg in relation to control group. The increased concentration of Arg in the urine of these patients would have a positive impact on the prophylaxis and therapeutic effects of our preventive treatment. The latter is of high importance, especially due to the fact that Arg is very similar in structure to proven complexing agents, such as ornithine, Na-EDTA (complexon III), etc.
This paper does not discuss the metabolic pathway of the Arginine.
Conclusion
The results of present study of Arg indicate a level of stone growth dissolution that considerably surpasses the one of any other amino acid. Our analysis proves that the positive impact of Arg on the CaOX dissolution is mainly due to the lower supersaturation of human urine, as a result of the administration of the agent. The “injection” of Arg to the human body through medication or diet could very effectively prevent the formation or further development of CaOX stones. Thus, we have assigned to Arg a promising place among the major solvents of CaOX calculi.
Disclosure
All the authors declared no competing interests.
| References | ▴Top |
- Ramello A, Vitale C, Marangella M. Epidemiology of nephrolithiasis. J Nephrol. 2000;13(Suppl 3):S45-50.
pubmed - Robertson WG. Renal stones in the tropics. Semin Nephrol. 2003;23(1):77-87.
doi pubmed - Binder HJ. Intestinal oxalate absorption. Gastroenterology. 1974;67(3):441-446.
pubmed - Grases F, Costa-Bauza A, Prieto RM. Renal lithiasis and nutrition. Nutr J. 2006;5:23.
doi pubmed - Tiselius HG. A hypothesis of calcium stone formation: an interpretation of stone research during the past decades. Urol Res. 2011;39(4):231-243.
doi pubmed - Messa P, Marangella M, Paganin L, Codardini M, Cruciatti A, Turrin D, Filiberto Z, et al. Different dietary calcium intake and relative supersaturation of calcium oxalate in the urine of patients forming renal stones. Clin Sci (Lond). 1997;93(3):257-263.
- Baumann JM, Affolter B, Caprez U, Henze U. Calcium oxalate aggregation in whole urine, new aspects of calcium stone formation and metaphylaxis. Eur Urol. 2003;43(4):421-425.
doi - Hammarsten G. On calcium oxalate and its solubility in the presence of inorganic salts with special reference to the occurrence of oxaluria. Comp-Rend Trav, Laboratoire Carlsberg: Copenhagen. 1921;17:1-29.
- Chow FC, Dysart MI, Hamar DW, Udall RH. Control of oxalate urolithiasis by DL-alanine. Invest Urol. 1975;13(2):113-116.
pubmed - Grimm U, Steinhauser I, Wulff K, Knapp A, Zschiesche M. Studies on tryptophan metabolism in calcium oxalate urolithiasis. Z Urol Nephrol. 1988;81(5):299-303.
pubmed - Fleming DE, van Bronswijk W, Ryall RL. A comparative study of the adsorption of amino acids on to calcium minerals found in renal calculi. Clin Sci (Lond). 2001;101(2):159-168.
doi - Atanassova S. Solubility and dissolution kinetics of calcium oxalate renal calculi in solutions, containing L-arginine: in-vitro experiments. J Crystal Growth. 2010;312:1940-1944.
doi - Boshev N. The biological constants in humans (in bulg). State Publishing House, Med i Fizk: Sofia. 1986:387-406.
- Gutzow I, Atanassova S, Budevsky G. Kinetics of dissolution of calcium oxalate calculi in physiological solutions containing Hippuric acid. Cryst Res & Technol. 1991;26(5):533-554.
doi - Gutzow I, Atanassova S, Neykov K. Solubility and Crystallization in biological fluids and the problems of life and health. Pure Apply Chem. 2002;74(10):1785-1792.
doi - Robertson WG, Peacock M, Nordin BE. Activity products in stone-forming and non-stone-forming urine. Clin Sci. 1968;34(3):579-594.
pubmed - Doremus RH, Teich S, Silvis PX. Crystallization of calcium oxalate from synthetic urine. Invest Urol. 1978;15(6):469-472.
pubmed - Leskovar P. Methoden und Techniken zum Erfassen der Kristalle in Wassrigen Losungen, unter besonderer Berucksichtigung der Problemstellugen in der Harnsteinforschung. Aktuell Nephrol. 1979;12:149-175.
- Ozturk H, Yagmur Y, Buyukbayram H. The effect of L-arginine methyl ester on indices of free radical involvement in a rat model of experimental nephrocalcinosis. Urol Res. 2006;34(5):305-314.
doi pubmed - Pragasam V, Kalaiselvi P, Sumitra K, Srinivasan S, Varalakshmi P. Counteraction of oxalate induced nitrosative stress by supplementation of l-arginine, a potent antilithic agent. Clin Chim Acta. 2005;354(1-2):159-166.
doi pubmed - Budevsky O. Foundation of chemical analysis. John Wiley & Sons: NY. 1979.
pubmed - Atanassova SS, Panchev P, Ivanova M. Plasma levels and urinary excretion of amino acids by subjects with renal calculi. Amino Acids. 2010;38(5):1277-1282.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.