

| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website http://www.wjnu.org |
Case Report
Volume 8, Number 1, March 2019, pages 17-18
An Atypical Case of Emphysematous Cystitis in a Young Non-Diabetic Patient
Behshad Charkhanda, Ali Kord Valeshabada, b, Joseph Farahanya, Jason Warnckea, Artineh Hayrapetiana, Mark R. Nehlera, Shandra Wilsona, c
aDepartment of Surgery, School of Medicine, University of Colorado Denver, Denver, CO, USA
bDepartment of Radiology, University of Chicago, Chicago, IL, USA
cCorresponding Author: Shandra Wilson, Department of Surgery, School of Medicine, University of Colorado Denver, 12631 E. 17th Ave., Room 560, Aurora, CO 80045, USA
Manuscript submitted October 16, 2018, accepted October 25, 2018
Short title: Emphysematous Cystitis in a Non-Diabetic Patient
doi: https://doi.org/10.14740/wjnu374
| Abstract | ▴Top |
Emphysematous cystitis is a rare, but severe infection of the urinary tract which is mostly found in older women with uncontrolled diabetes. A 34-year-old non-diabetic male with a past medical history of refractory hepatic encephalopathy presented with fever and increased lower abdominal pain for 1 day. Computed tomography (CT) scan demonstrated multiple gas foci in a diffuse collection of gas within the thickened bladder wall suggestive of emphysematous cystitis, and urine culture revealed Klebsiella pneumoniae as the causative agent. The infection resolved with bladder drainage and irrigation and antibiotic therapy in 1 week. An atypical case of emphysematous cystitis in a young non-diabetic man is reported. Early diagnosis and prompt treatment are essential to achieving a favorable prognosis and to preventing a potentially fatal condition.
Keywords: Emphysematous cystitis; Urinary tract infection; Pneumaturia; Computed tomography
| Introduction | ▴Top |
Emphysematous cystitis is a very rare and complicated urinary tract infection which is characterized by air within the bladder wall and lumen caused by underlying gas-producing bacterial infection. The disease is mostly found in elderly diabetic women with variable clinical presentation which can rapidly progress to a life-threatening condition. The etiology of the disease is not well understood. Abdominal computerized tomography (CT) is the most sensitive and specific diagnostic tool [1-3]. We report an atypical case of emphysematous cystitis in a young non-diabetic man who presented with increased abdominal pain and fever.
| Case Report | ▴Top |
The patient was a 34-year-old male with a past medical history of ethanol-induced cirrhosis and refractory hepatic encephalopathy. He presented to the emergency department with fever and increased lower abdominal pain for 1 day. The patient had chronic pain due to ascites, but the new pain was described as the worst pain he has experienced, and was associated with objective fever and chills. The patient had a previous history of urinary catheterization during his previous hospitalization 2 weeks before the current admission. The patient’s past medical history included cirrhosis, hepatic encephalopathy, thrombocytopenia, spontaneous bacterial peritonitis, esophageal varices, and a prior inguinal hernia repair. His medications included furosemide, lactulose, omeprazole, rifaximin, simethicone, spironolactone, sulfamethoxazole-trimethoprim, tramadol, zinc sulfate and multivitamins.
On admission, vital signs showed fever (temperature 38.7 °C), tachycardia (pulse rate 135 beats/min), and tachypnea (respiratory rate 28/min). His blood pressure was 132/69 mm Hg. Physical examination revealed mild icterus sclera, abdominal distension and abdominal tenderness, particularly in the peri-umbilical region. Laboratory testing revealed white blood cell (WBC) count of 2.8 × 109/L, hemoglobin of 10.4 g/dL, platelet count of 59 × 109/L, and lactate level of 3.6 mmol/L. Urine analysis disclosed leukouria, bacteruria and 11 - 30 red blood cells per field. Because of the abdominal findings, a CT scan of the abdomen and pelvic was performed, which demonstrated multiple non-dependent gas foci within the thickened bladder wall, suggestive of emphysematous cystitis (Fig. 1a).
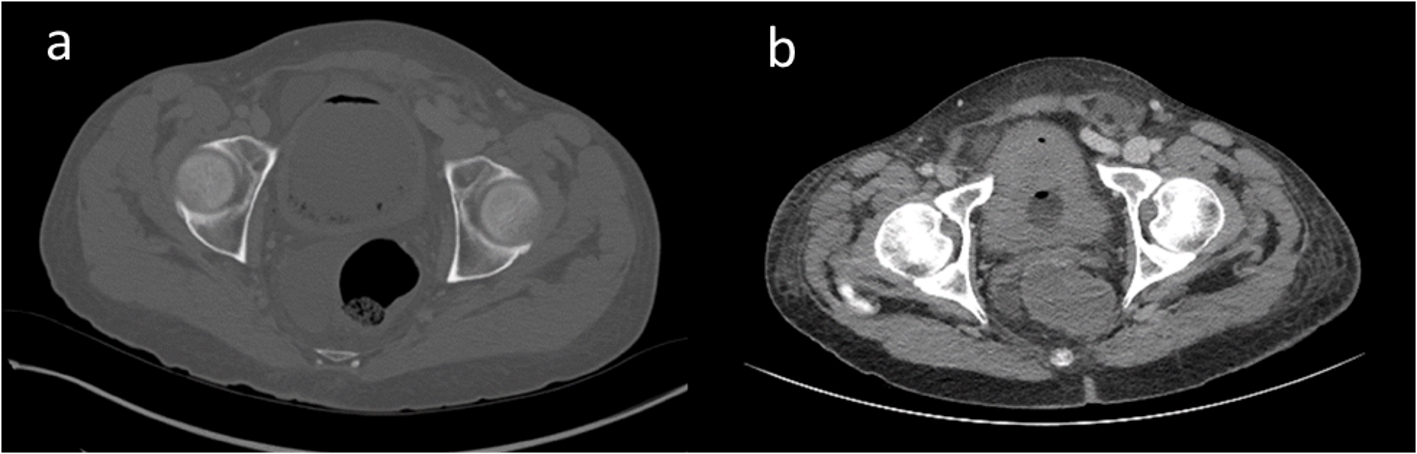 Click for large image | Figure 1. Computed tomography at admission showed multiple non-dependent gas foci within the thickened bladder wall suggestive of emphysematous cystitis (a) which was markedly improved following catheter decompression and antibiotic therapy (b). |
Blood and urine cultures confirmed Klebsilla pneumonia as the causative agent. Antibiotic therapy started with piperacillin-tazobactam in addition to fluid resuscitation and bladder decompression with catheter reinsertion. At 7 days, a follow-up CT scan delineated a markedly improved appearance of emphysematous cystitis following catheter decompression (Fig. 1b). Antibiotic was transitioned to ceftriaxone, and indwelling catheter was removed. A high-grade fever, however, developed, which was ultimately attributed to possible beta-lactam drug reaction following negative repeated infectious work-up. Within 24 h of starting levofloxacin, fevers resolved. Finally, the patient was discharged to home with oral levofloxacin regimen to complete a 14-day course.
| Discussion | ▴Top |
Emphysematous cystitis is a rare, but severe infection of the urinary tract. Although older women with uncontrolled diabetes are at the highest risk for developing emphysematous cystitis [4], the patient in this study was a young man without diabetes. Other known risk factors include chronic urinary retention/obstruction (neurogenic bladder, diabetic, prostatic hypertrophy or urethral stricture), presence of renal transplantation, chronic indwelling urinary catheters, endoscopic urologic procedures, chronic urinary tract infection, systemic lupus, immunosuppression due to corticosteroids, and immunosuppressive agents with bladder toxicity such as cyclophosphamides [1-4]. The patient in this study had decreased WBC count and a previous history of urinary catheterization in the previous hospitalization which may have predisposed him to the development of this infection.
Laboratory testing demonstrates positive urine cultures with E. coli or Klebsiella pneumoniae in 80% of the cases of emphysematous cystitis [4], just as we found in our patient. Imaging, particularly CT scan, has a key role in the diagnosis and assessment of the disease, characterized by multiple non-dependent gas foci within the thickened bladder wall, as observed in our case [5]. Bladder catheterization for optimal drainage and irritation with antibiotic therapy and blood glucose control are recommended treatment for emphysematous cystitis, resolving the infection in majority of cases as observed in this patient. Emphysematous cystitis is a life-threatening disease and may result in urosepsis and even death in up to 7% of the cases [2, 3].
In summary, an atypical case of emphysematous cystitis in a young non-diabetic man was reported. Early diagnosis and prompt treatment are essential to achieving a favorable prognosis and to preventing a potentially fatal condition.
Conflict of Interest
None of the author has conflict of interest to declare.
Financial Support
None.
| References | ▴Top |
- Grupper M, Kravtsov A, Potasman I. Emphysematous cystitis: illustrative case report and review of the literature. Medicine (Baltimore). 2007;86(1):47-53.
doi pubmed - Bjurlin MA, Hurley SD, Kim DY, Cohn MR, Jordan MD, Kim R, Divakaruni N, et al. Clinical outcomes of nonoperative management in emphysematous urinary tract infections. Urology. 2012;79(6):1281-1285.
doi pubmed - Mokabberi R, Ravakhah K. Emphysematous urinary tract infections: diagnosis, treatment and survival (case review series). Am J Med Sci. 2007;333(2):111-116.
doi pubmed - Amano M, Shimizu T. Emphysematous cystitis: a review of the literature. Intern Med. 2014;53(2):79-82.
doi pubmed - Grayson DE, Abbott RM, Levy AD, Sherman PM. Emphysematous infections of the abdomen and pelvis: a pictorial review. Radiographics. 2002;22(3):543-561.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.