

| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website https://www.wjnu.org |
Case Report
Volume 10, Number 1, September 2021, pages 12-14

Large Renal Cyst Underestimates Split Function on Diuretic Radionuclide Renal Scan
Shrikant V. Solava, Shailendra V. Savalea, b
aSPECT Lab, Nuclear Medicine Services, Pune, Maharashtra, India
bCorresponding Author: Shailendra V. Savale, Dr. Solav’s SPECT Lab, Bavdhan, Pune, Maharashtra 411021, India
Manuscript submitted December 23, 2020, accepted June 12, 2021, published online September 28, 2021
Short title: Large Renal Cyst Underestimates SRF
doi: https://doi.org/10.14740/wjnu422
| Abstract | ▴Top |
Radionuclide renal scan performed with (diethyle triamine penta acetic acid (DTPA), ethylene dicysteine (EC), mercaptoacetyltriglycine (MAG3), and dimercaptosuccinic acid (DMSA) provides split function between the two kidneys. Hence it is a valuable method to evaluate percentage function prior to nephrectomy. Nephrectomy may be done in a prospective renal donor or it may be done for a diseased kidney. In either case, the nephrologist/ urologist must ensure that the remaining kidney is able to sustain renal function post nephrectomy. We present a case where conventional renal scan had underestimated the split function due to a large posterior cortex cyst accounting for attenuation of radionuclide photons. Repeat scan in anterior view had eliminated this erroneous result. We could not find any such reported discrepancy despite extensive web-based search.
Keywords: Radionuclide renal scan; DTPA; Split renal function
| Introduction | ▴Top |
Radionuclide renal scan is a time-tested method to assess split renal function (SRF). It is deciding test prior to donor nephrectomy [1]. SRF is usually calculated by quantifying the radiotracer counts in the two kidneys between 2 and 3 min using computer-generated renogram. Several factors account for variation in split function such as body habitus, location of kidney (patient factor) and placement of region of interest, background subtraction (operator dependent factors), etc. A variation of 2-7% in the same patient on follow-up scan has been reported [2]. Various radionuclides have been used to estimate SRF. These are technetium (Tc)-99m-diethyle triamine penta acetic acid (DTPA), Tc-99m-mercaptoacetyltriglycine (MAG3), Tc-99m-dimercaptosuccinic acid (DMSA). Computed tomography (CT) angiography and dynamic contrast-enhanced magnetic resonance (MR) angiography have also been used to calculate SRF [3, 4]. An 80-year-old male was detected with renal mass on sonography. CT scan revealed an enhancing tumor in the interpolar region of left kidney. Tc-99m-DTPA renal scan showed compromised function of right kidney both qualitatively and quantitatively. The CT scan was reviewed and there was a large cyst in the posterior cortex of right kidney. Hence, the radionuclide scan was repeated in anterior view on another day (within 1 week). The repeat scan showed equal split function of the two kidneys. Thus, it is important to recognize that structural changes may result in misinterpretation of renal scan. Adequate precautions observed prior to imaging may prevent such errors.
| Case Report | ▴Top |
An 80-year-old male had vague pain in abdomen. He was hemodynamically stable. General examination was normal.
His sonography revealed a mass in lower pole of left kidney. CT showed a solid lobulated lesion at the lower and interpolar cortex of the left kidney with heterogeneous post contrast enhancement suggesting renal neoplasm. An exophytic cortical cyst at interpolar cortex of the right kidney was also noted. His biochemical profile was normal. Serum creatinine was 0.91 mg/dL.
Radionuclide renal scan was performed in conventional posterior view using 4 mCi of Tc-99m- DTPA administered intravenously with simultaneous acquisition of dynamic renal scan at the rate of 1 min per frame for 20 min. Siemens single head E-cam gamma camera system was used with low energy high resolution collimator. Split function was assessed using computer-generated renogram. Region of interest was drawn by an experienced operator. The split function calculated was 82% from the left kidney and 18%from the right kidney (Fig. 1a). As the structural appearance of the kidneys was quite normal on CT urography (Fig. 2a), and in view of a large cyst located on the posterior cortex of right kidney (Fig. 2b, c), the Tc-99m-DTPA renal scan was repeated in anterior view on another day.
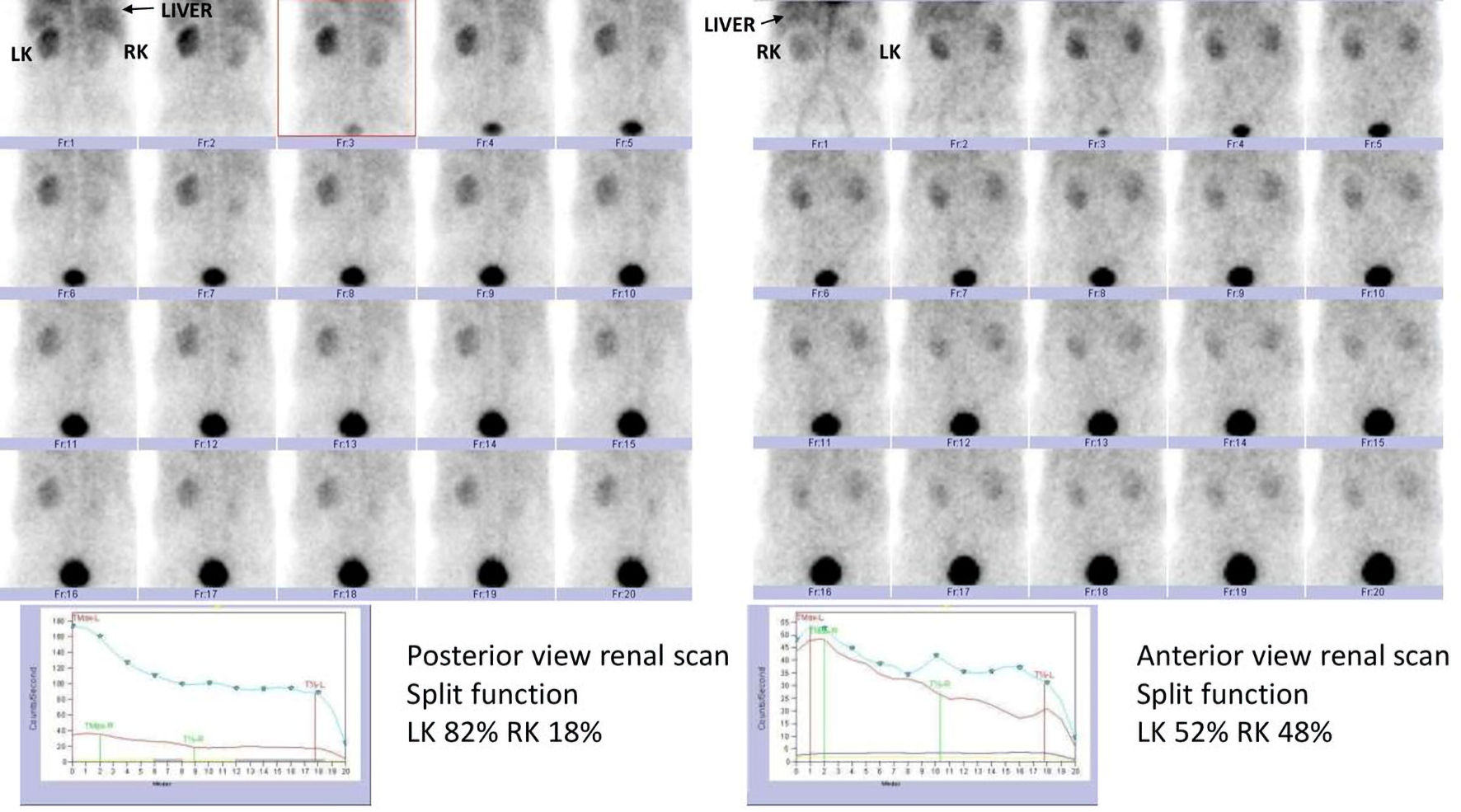 Click for large image | Figure 1. (a) The split function calculated by Tc-99m-DTPA renal scan in conventional posterior view. The split function calculated was 82% from the left kidney and 18% from the right kidney. (b) Tc-99m-DTPA renal scan was repeated in anterior view on another day. The repeat scan showed equal distribution of radiotracer qualitatively on sequential images. The split function calculated was 52% from the left kidney and 48% from the right kidney. Tc: technetium; DTPA: diethyle triamine penta acetic acid. |
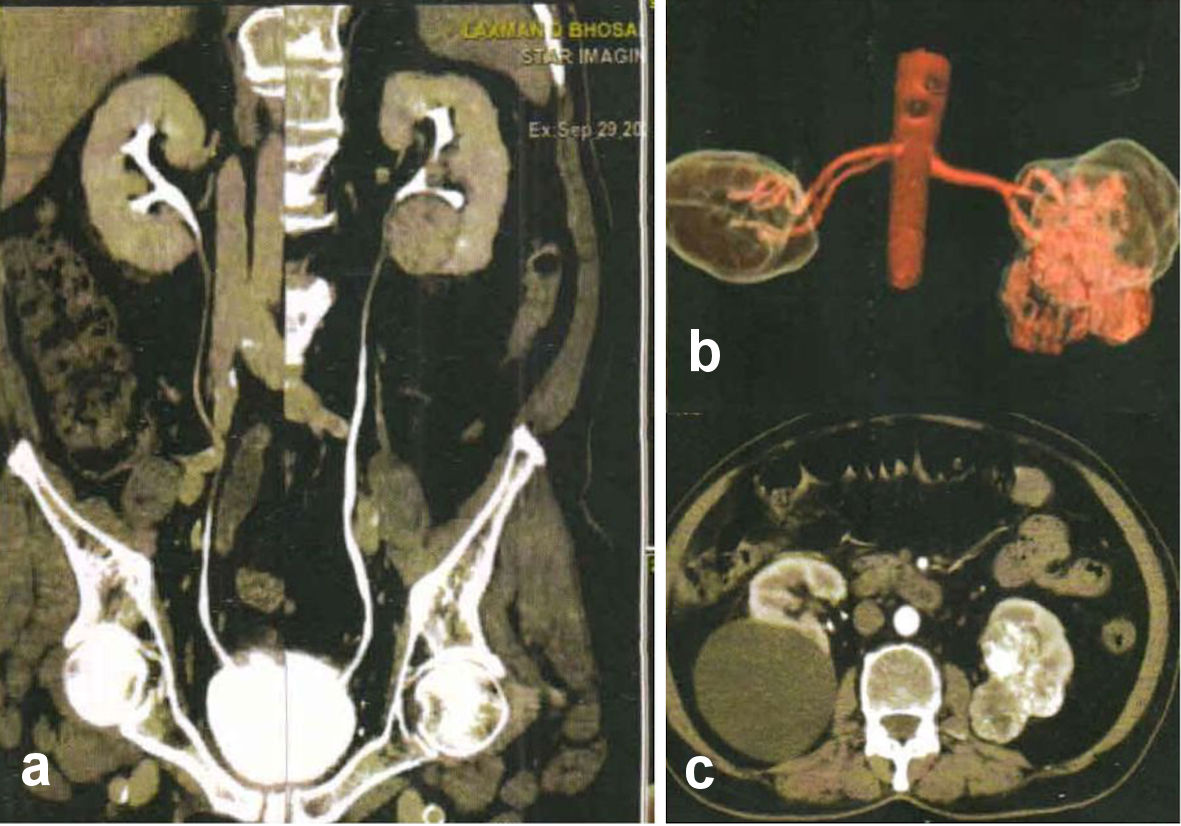 Click for large image | Figure 2. (a) Normal structural appearance of the kidneys on CT urography. (b, c) A large cyst located on the posterior cortex of right kidney. CT: computed tomography. |
The repeat scan showed equal distribution of radiotracer qualitatively on sequential images (Fig. 1b). The glomerular filtration rate (GFR) calculated by Gates protocol showed satisfactorily functioning kidneys.
| Discussion | ▴Top |
The gold standard for assessment of renal function is GFR [5]. This must be done with inulin clearance, and is tedious and impractical for routine use on patients. Inulin is freely filtered by the kidneys. It is neither secreted nor reabsorbed by the tubules, and it is not metabolized [6]. A surrogate marker is creatinine clearance that measures the ability of the kidneys to clear creatinine from the circulation in 24 h.
Serum creatinine is by far the easiest and first test to assess renal function. However, serum creatinine subject to physiologic variation depending on muscle mass (high muscle mass overestimates) and age (elderly may have false low estimates). However, the GFR must fall below 50% before there is rise in serum creatinine level. Thus, an elevated value clearly indicates compromised renal function, but a normal value does not eliminate need for further assessment of renal function [7]. Risk of chronic renal failure following radical nephrectomy is well known [8]. SRF using renal scintigraphy has been recommended when the creatinine is high, the GFR is low and where there are multiple renal tumors. Radionuclide renal scan is an important method to assess renal function when nephron sparing surgery is performed [9]. Dynamic renal scintigraphy can be performed using Tc-99m-DTPA, Tc-99m-EC, Tc-99m-MAG3, and iodine-123 orthoiodohippurate. DTPA is the only agent that is purely filtered by the glomeruli. EC, MAG3 and hippuran are also secreted by the tubules, and hence are not suitable for assessment of GFR [10]. Errors in estimation of split function have been described due to high background activity in mild renal insufficiency [11]. Adequate precautions while processing the scan such as using correct frames for drawing the region of interest may overcome this issue. However, we did not come across any reference where a renal cyst underestimates the split function because of its position causing attenuation of photons. Our case highlights this particular aspect. A large posterior cortex renal cyst gives rise to blunted radionuclide counts (attenuation) in conventional posterior view of renal scan. Change of acquisition to anterior view eliminates with artifact.
Geist et al have reported estimation of split function using 18-F fluorodeoxyglucose (FDG) by positron emission tomography (PET) MR, and compared the results with Tc-99m-MAG3 scan. Despite of difference in pharmacokinetics, their results showed good correlation between the two-radiotracer methods in estimation of split function, mean transit time and output efficiency [12]. Radionuclide renal scan is a useful method to assess renal function. It is required to assess split function prior to nephrectomy or nephron sparing surgery. However, it does not provide adequate structural information. Hence, it is important to know the structure of kidneys for accurate estimation of split function and obviate errors as demonstrated in this case report.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
Shrikant V. Solav as the guarantor contributed to the study design, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, and manuscript editing. Shailendra V. Savale contributed to the concepts, definition of intellectual content, literature search, data acquisition, statistical analysis, manuscript preparation, and manuscript review.
Data Availability
The authors declare that data supporting the findings of the study are available within article.
| References | ▴Top |
- Shokeir AA, Gad HM, el-Diasty T. Role of radioisotope renal scans in the choice of nephrectomy side in live kidney donors. J Urol. 2003;170(2 Pt 1):373-376.
doi pubmed - Lin WY, Changlai SP, Kao CH. Normal ranges of renal physiological parameters for technetium-99m mercaptoacetyltriglycine and the influence of age and sex using a camera-based method. Urol Int. 1998;60(1):11-16.
doi pubmed - Summerlin AL, Lockhart ME, Strang AM, Kolettis PN, Fineberg NS, Smith JK. Determination of split renal function by 3D reconstruction of CT angiograms: a comparison with gamma camera renography. AJR Am J Roentgenol. 2008;191(5):1552-1558.
doi pubmed - Claudon M, Durand E, Grenier N, Prigent A, Balvay D, Chaumet-Riffaud P, Chaumoitre K, et al. Chronic urinary obstruction: evaluation of dynamic contrast-enhanced MR urography for measurement of split renal function. Radiology. 2014;273(3):801-812.
doi pubmed - Davidson A, Cameron J, Grinfeld JP, et al. Renal function and testing of function. Oxford textbook of clinical nephrology. 1998.
- Cole BR, Giangiacomo J, Ingelfinger JR, Robson AM. Measurement of renal function without urine collection. A critical evaluation of the constant-infusion technic for determination of inulin and para-aminohippurate. N Engl J Med. 1972;287(22):1109-1114.
doi pubmed - Levey AS, Becker C, Inker LA. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: a systematic review. JAMA. 2015;313(8):837-846.
doi pubmed - Huang WC, Levey AS, Serio AM, Snyder M, Vickers AJ, Raj GV, Scardino PT, et al. Chronic kidney disease after nephrectomy in patients with renal cortical tumours: a retrospective cohort study. Lancet Oncol. 2006;7(9):735-740.
doi - Uzzo RG, Novick AC. Nephron sparing surgery for renal tumors: indications, techniques and outcomes. J Urol. 2001;166(1):6-18.
doi - Blaufox MD, Aurell M, Bubeck B, Fommei E, Piepsz A, Russell C, Taylor A, et al. Report of the Radionuclides in Nephrourology Committee on renal clearance. J Nucl Med. 1996;37(11):1883-1890.
- Sennewald K, Taylor A, Jr. A pitfall in calculating differential renal function in patients with renal failure. Clin Nucl Med. 1993;18(5):377-381.
doi pubmed - Geist BK, Baltzer P, Fueger B, Hamboeck M, Nakuz T, Papp L, Rasul S, et al. Assessment of the kidney function parameters split function, mean transit time, and outflow efficiency using dynamic FDG-PET/MRI in healthy subjects. Eur J Hybrid Imaging. 2019;3(1):3.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.